This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
On a recent shift, I received sign-out for Room 20, a 46 year old man with a history of schizophrenia as well as alcohol and cannabis abuse. He came to us from a nursing home where he lives. He accidentally set his room on fire with a cigarette, prompting the nursing home to kick him out for being a risk to the facility. Although he had no acute medical issues, he was sent to the emergency department so “the health care system” could find him a new home.
Following up with another 35 “diseases just learned.” Please look back to last week’s intro if you are just coming to this series. Like Part I, this is a gift to our paid subscribers. This Substack is reader-supported. If you appreciate our work, consider becoming a free or paid subscriber.
John and Adam discuss our hopes for Vinay’s tenure at the FDA and how we intend to keep Sensible Medicine a vibrant place on Substack, a place where we will continue to showcase a range of ideas and opinions about all things bio-medicine. We also answer some of the questions from our recent “ask us anything” post.
I enjoyed reading the comments on yesterday's post regarding the positive results of the ESSENCE trial of semaglutide vs placebo in patients with metabolic dysfunction-associated steatohepatitis (MASH). Thank you to those who took the time to write. I wanted to share some very brief thoughts on two basic tenets of medical practice that emerged from the thoughtful commentary.
Three professors, writing in the Lancet , estimated that the global prevalence of the condition is 25%. A modeling study predicted that its prevalence will rise sharply in the coming decade. The condition has a terrible name. It’s called metabolic dysfunction-associated steatohepatitis (MASH). That’s its new name. The old names, non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH) were not much better.
One of the many great things about being a general internist is the exposure to the wondrous diversity of humanity. I am a better person for having brief, but intense, visits with some 50 people every week. These people grew up all over the world and have worked in every imaginable field. I see people barely scraping by financially and people with unimaginable wealth.
The most common question we get asked is: is there a course on how to become better at critically reading medical research. Well, now there is! This is the first of 9 videos that we recorded as part of a course on clinical appraisal, and there will be many more to come. We call our class: How Not to Get Fooled by the Medical Literature. These are topics that each of us teaches separately, but, here, for the first time, we teach them together, and the whole is more than the sum of the parts.
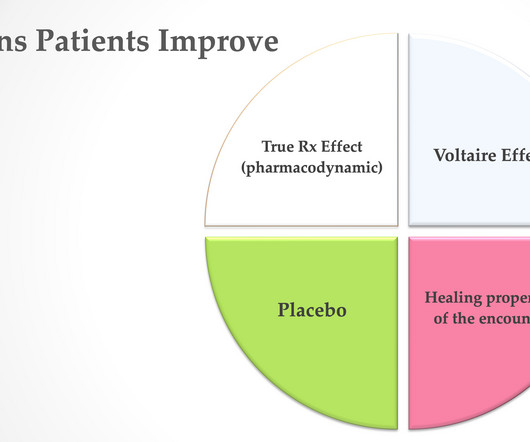
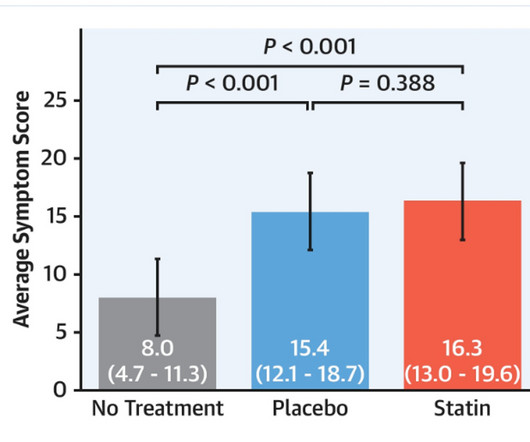
The picture below shows how a treatment can make patients better. I see four ways. The drug/procedure may work biologically. The Voltaire effect relates to his quote saying that the art of medicine consists of amusing the patient while nature cures the disease. AKA: natural history. Placebo effects can also contribute. I will show you an elegant experiment demonstrating how positive energy and words can add to improvement.
For me, transcatheter aortic valve implantation (TAVI) approaches a miracle. My brain thinks: how in the world does a doctor place a valve in the aorta, then into the stenotic valve, squish the calcified old valve and land a new one. Watching the procedure on x ray does not do the miracle justice. Miracle number one is the valve stays in place. Miracle number two is that the debris-traveling-north does not cause stroke in every patient.
Not every week, but most weeks I read social media posts about getting your heart checked. It could be lifesaving. The pleas often start with a coronary artery calcium scan—which could then lead to a coronary angiogram with possible stent placement. It’s a compelling story. Heart disease is a leading killer. Sudden cardiac death or massive heart attack can be the first symptom.
I’ve already gotten pretty bored reading about AI in medicine. So many of the articles cover the same ground, either breathlessly celebrating AI’s promise or bemoaning the brave new world on the horizon. This article from Dr. Mendoza made me feel embarrassed that I have not even considered this angle. Adam Cifu This Substack is reader-supported.
In the Spring of 2008, I was stationed aboard the La Rabida Children's hospital. The hospital was perched on a peninsula that jut into Lake Michigan on Chicago's South Side. Outside all the windows spilled tranquil blue water. We could have been in the Pacific. The patients were a mix of kids who were hospitalized for a treatable conditions, like diabetic keto acidosis, as well as those who were incurable, like a cute 2 year old boy with a brain stem tumor that grew relentlessly after neurosurge
I’m obviously a big fan of reflective writing and of “advice columns.” So, when I got a submission that combines the two genres, and was written by an internal medicine resident, it was impossible not to share. Adam Cifu This Substack is reader-supported. If you appreciate our work, consider becoming a free or paid subscriber. Medical students around the country recently celebrated the annual tradition of Match Day, where graduating students learn where they have “matched
I want to start a new series on Sensible Medicine. It’s called: I Learned about Medicine From That; These are first hand accounts since I started in medicine in 2005. This is about the first patient I took care of who died. -Vinay Prasad This Substack is reader-supported. To receive new posts and support our work, consider becoming a free or paid subscriber.
Stadiums packed with working-class Americans cheering for public health. Political leaders calling for war on our chronic disease crisis. An incoming NIH Director, Jay Bhattacharya M.D., Ph.D. committed to reform. Had someone painted this picture when I was a graduate student at the Johns Hopkins Bloomberg School of Public Health where the moto is “saving lives, millions at a time” it would have sounded like a dream come true.
One of my patients recently had an executive physical. The eight-page report arrived in my in-basket. This happens regularly enough, two or three times a month, that it shouldn’t bother me anymore. This essay is about why it still does. This Substack is reader-supported. To receive all posts, consider becoming a paid subscriber. I joke that my practice has evolved to become a selective one.
Regular readers of Sensible Medicine will understand that this post by Rebecca Silverman needs no introduction. Adam Cifu Sensible Medicine is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber. Every 5-7 years, we each have to renew our licenses and passports, take our cars for inspections, replace major home appliances, or hire a contractor to fix a broken pipe.
Colton Lipfert is an incoming medical student at an east coast medical school. He has worked in the vkprasadlab for the last few years and recently shadowed. When I finished shadowing Dr. Vinay Prasad, I was convinced I had to become an oncologist. When I told him this, he was a little surprised. The day’s work had been downright ordinary for him.
“Don’t worry about reading – you won’t be able to keep your eyes open. The only thing you need to learn this year is how to differentiate sick people from not sick people.” So said my program director during my internship. This comment might be one of the reasons I’ve been skeptical of sepsis screening. If there is one thing a medicine resident or hospitalist should be able to do well is identify the patients who are sick and need attention.
Marty Makary's book "Blind Spots" seems to be popular among Sensible Medicine readers. Dr. Joseph Rall found one part that he didn't think adequately represented current practice. Here he discusses the most recent data regarding the safety of planned home birth in selected women. Thanks for reading Sensible Medicine! This post is public so feel free to share it.
The Journal of the American Medical Association published an actual randomized controlled trial for coronary artery calcium (CAC). As a skeptic of this imaging test, I saw the headline and thought: finally, we will learn whether patients who have their chest radiated have better outcomes. Better outcomes, such as fewer heart attacks or strokes, or longer life, is why we interact with healthcare.
FH is a 66-year-old woman who comes in for an urgent visit because she has been feeling woozy for two days. She is very anxious, almost distraught, because she thinks these symptoms are the same as the ones that her sister had before she died of a hemorrhagic stroke. Sensible Medicine is a reader-supported publication. If you appreciate our work, consider becoming a free or paid subscriber.
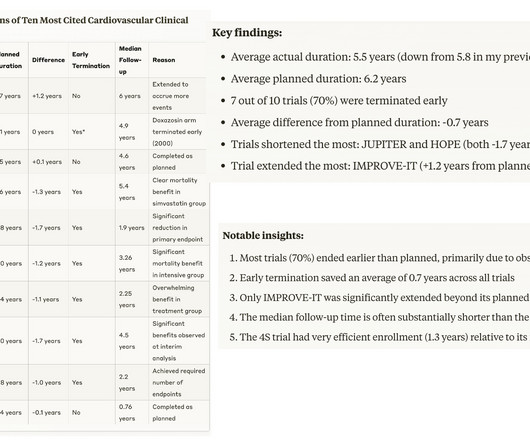
Co-editor of Sensible Medicine Vinay Prasad and two colleagues published a remarkable study last week regarding the length of antidepressant drug trials vs duration of therapy in the real world. The median trial duration was 8 weeks while real-world use of these drugs is 5 years. Few trials lasted long enough to monitor for withdrawal symptoms or included taper protocols.
As always, we are happy to feature articles that expand on ideas discussed on Sensible Medicine – even when the author agrees more with Dr. Prasad than with me. Today, we welcome back Dr. Raudasoja, who last published with us about a year ago. Adam Cifu Sensible Medicine is a reader-supported publication. If you appreciate our work, consider becoming a free or paid subscriber.
John is sick, so I have big shoes to fill. Today’s study of the week is a cancer trial. I know many of you aren’t cancer doctors, and you are thinking about skipping this essay. Let me assure you: you will learn something. The trial has issues with control arm, skewed randomization (2:1), drop out and endpoints. It is a rollercoaster ride of critical appraisal.
Pitchers and catchers. George Vecsey probably said it best. Just say it out loud, the mantra that gets some of us through the winter. Pitchers and catchers, pitchers and catchers. Like NPR republishing Susan Stamberg's cranberry relish recipe or every dance school putting on The Nutcracker each December, I think Sensible Medicine needs a tradition. So here, in honor of the start of spring training, when pitchers and catchers report for duty, a Friday Reflection that I first posted on Feb 17, 202
What we expect students to do to get into medical school -- and then match into a desirable residency -- is absurd. Why do we do this? Because we won’t admit that we can’t predict who will be a successful doctor. Because there are too many good applicants for the spots we have. Because we are too lazy, or cheap, to invest the time and energy to get to know our applicants.
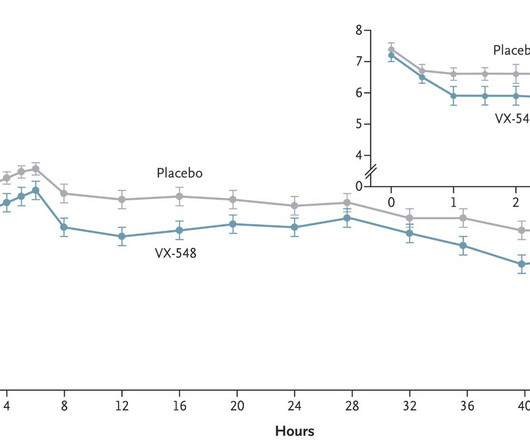
Last week the FDA approved a novel non-opioid pain medication. The drug is called suzetrigine (Journavx). A Google search brings up news releases from Vertex , and news coverage—which are essentially the same and lacking links to the evidence. I aimed to provide readers the evidence for this new drug. This was much more difficult to find. Some things to set out first: I am not a pain specialist; my analysis is one of a Neutral Martian.
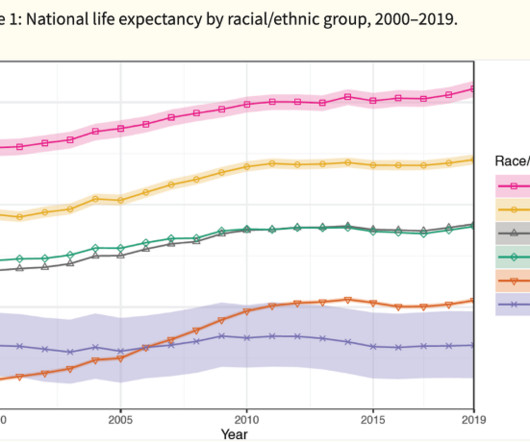
About ten years ago, I decided that I didn’t want to hear about race in the chief complaint of clinical presentations. 1 Instead of “The patient is a 35-year-old African American male with cough, fever, and sputum production;” I wanted “The patient is a 35-year-old man with cough, fever, and sputum production.” Sensible Medicine is a reader-supported publication.
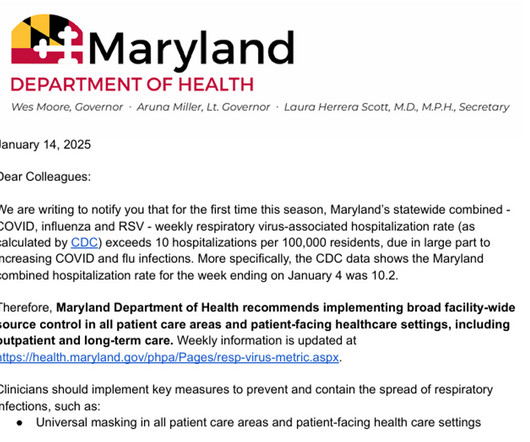
A limited mask mandate is returning to my state this week. In 2023, the Maryland Department of Health (DOH) adopted a standard for return to universal masking in healthcare facilities when hospitalizations with respiratory viruses (covid, influenza, or RSV) reach a level of 10 cases per 100,000 population. Maryland has a population of 6.3 million and about 10,000 licensed hospital beds, so that works out to about 6% of hospital beds.
Doctors seek therapies that reduce the chance of bad outcomes. When treating patients with suspected coronary disease, typical bad outcomes to prevent are myocardial infarction (MI) and death due to heart disease. This usually requires drugs or interventions, such as urgent percutaneous coronary intervention (PCI) with stents during an acute MI. (PCI in stable disease does not reduce events.
Two health obsessions that I’ve never really understood are the supposed benefits of vitamin D (for every imaginable ill) and harm of seed oils. Dr. Bobby Dubois thinks a lot about the evidence behind health recommendations on his podcast. His research has led him to a pretty clear opinion about the role of seed oils in health and disease. Attentive Sensible Medicine readers will note that his take is a bit different from that expressed in a recent post.
Atrial fibrillation is one of the most common reasons people get admitted to a hospital. As Western society grows larger and less active, AF incidence continues to rise. In short, few questions in cardiology are more relevant than the treatment of patients with new-onset AF. There are two paths of treating patients with AF. (After initiation of stroke prevention regimens—often with oral anticoagulation.
Frequently, after a school shooting, The Onion publishes the headline , “‘No Way To Prevent This,' Says Only Nation Where This Regularly Happens." 1 I find this a brilliant response. Admittedly, less brilliant is my response every time the media predictably starts reporting on a “motive”: “Why are people looking for a motive?
Last week, I expanded on my nine pieces of “Advice for Internship.” As I noted, a little over a year ago I updated this list after an inpatient attending block during which I was reminded just how hard it is to be an intern. Part II is a bit less pithy, more parochial, but maybe more useful than Part I. The advice might be a bit internal medicine oriented, but I do think it is broadly applicable.
Distinguishing between diseased and healthy states in medicine has immense consequences because it influences treatment, insurance coverage, employment, and disability. But this distinction is arbitrary since health exists on a continuous spectrum. The people whose diagnostic test result is a few smidgeons on the ‘healthy’ side of the line are meaningfully no different than those a few smidgeons on the ‘diseased’ side.
Nearly a thousand news outlets covered the recent publication of the positive results of the STEP-9 trial of semaglutide vs placebo for the treatment of knee pain due to osteoarthritis in patients with obesity. Twitter overflowed with positive messages after the New England Journal of Medicine publication. I am not sold on the trial. STEP-9 had many flaws but one fatal flaw.
It goes without saying that we at Sensible Medicine pray at the church of Evidence-Based Medicine. Fields of medicine vary in how strong the “best available evidence from systematic research” leg of the three-legged stool is. If you are a cardiologist, you might be able to rely heavily of RCTS. Some other fields, with a weaker evidence base, might have to lean heavier on basic science or clinical experience and “N of 1” trials.
The study of the week will take a short break. I head to Curitiba Brazil tomorrow for the Brazilian EP society meeting. I have five lectures. I will be back next week. And there will be plenty of studies to choose from because we are entering the fall season of medical meetings. This week, Sensible Medicine features a guest column from Zachary R. Caverley, a Cardiology Physician Assistant working in the Northwest coast of Oregon.
Most of the voices on Sensible Medicine are doctors and patients. This is a bit of a shame as so many people are involved in and work on healthcare and healthcare policy. We are thrilled to feature this article from three legal scholars. The essay outlines a recommendation for how we can encourage better post approval research. This piece is just a taste of the work they are doing.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content