This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Building a Better Health Record (BBHR) As part of our documentation quality improvement initiative , we promote practical ways for clinicians to provide clear and actionable communication at transitions of care.
Building a Better Health Record (BBHR) As part of our documentation quality improvement initiative , we promote practical ways for clinicians to provide clear and actionable communication at transitions of care.
In the case of house calls , physicians need to document that the home visit was medically necessary. Here are a few reminders to consider before you bill for a house call: Providers need to document if the home visit is based upon a one-time, ongoing, or permanent need. These can be documented and billed in addition to the visit code.
This left shift of activity forms a key component of this plan, which seeks to create capacity in secondary care in part by moving activity into primary care. What can we learn about the left shift of activity from this document? to 4M, with a payment of 20 per advice and guidance request for general practice attached.
These systems offer significant advantages in data consistency and workflow efficiency, as clinical documentation automatically flows into billing processes without manual intervention. The system should offer RESTful APIs with comprehensive documentation and developer support.
In 2027, at least 80% of electronic prior authorization approvals (with all needed clinical documentation) will be answered in real-time. These changes will be operational for fully insured and commercial coverage by Jan. 1, 2026, with a focus on supporting regulatory changes for expansion to additional coverage types.
Healthcare training in North Carolina emphasizes the development of strong decision-making skills, empowering trainees to evaluate patient needs and implement appropriate careplans efficiently. With training, trainees learn how to operate complex machinery, conduct accurate testing, and maintain meticulous records.
Unlike conventional AI models that rely solely on their training data, RAG combines the power of large language models with real time information retrieval from your organization’s specific databases and documents. Here’s the proven roadmap we’ve developed through multiple healthcare RAG deployments.
The business case should quantify expected benefits including improved clinical efficiency, reduced documentation burden, enhanced patient safety through clinical decision support, and operational cost savings through workflow optimization. Epic configuration should accommodate both in-person and virtual care workflows.
This includes a Clinical AI Agent, AI-driven insights at the point of care, AI-powered summaries, and personalized careplans. Even today, as Seth Joseph documents , Epic is already attracting lawsuits from multiple “smaller, adjacent vendors.”
By using Success, Effort, Emotion, and Trust (SEET) as measurements for every PX processfrom appointment setting to careplans to paymentsthe healthcare community can expand its potential for providing excellent care. No touchpoint is too small for inclusion.
Challenge #2 – The Dreaded Last-Minute Cancellation Even after securing a clinical placement, nurse practitioner students face another potential crisis: the last-minute preceptor cancellation, which can derail carefully planned educational journeys with little warning. Missing one rotation can delay an entire course sequence.
Canceling services and coordinating mail forwarding are important tasks to prevent unnecessary expenses and ensure receipt of important documents. SHOW MORE Transitioning your medical practice takes carefulplanning, communication and the right professional support. This is where a broker or appraiser comes in.
Balancing Administrative Duties with Clinical Work Challenge: Administrative responsibilities, such as documentation and billing, can detract from direct client work. Clearly define roles and responsibilities in collaborative settings, and maintain open communication to ensure cohesive careplans.
Things like: Clinical documentation and note-taking Prior authorization paperwork Appointment scheduling and reminders Medical coding and billing While physician burnout has declined in recent years, almost half of clinicians still report feeling stressed.
Clear, consistent documentation and communication with both patients and referring providers can help ensure follow-up and appropriate careplanning. Better reporting leads to better outcomes Another priority is standardizing radiological reporting for emphysema identified during lung cancer screening.
As healthcare systems become more complex, physicians are spending more time on administrative tasks, including clinical documentation. Team documentation is a powerful way to streamline patient visits and EHR data entry so the entire team can focus on delivering excellent care. What is team documentation?
Best billing practices for Alzheimer’s and Dementia Care 1. Thorough documentation Comprehensive documentation is the cornerstone of successful medical billing for Alzheimer’s and dementia care. It also supports high-quality patient care.
Another name for this is advance careplanning. It includes a) clarifying a patient’s understanding of their illness and its treatments, b) understanding their goals of care and c) learning what is important to them. To receive new posts and support our work, consider becoming a free or paid subscriber.
Coding and clinical documentation have never been more important in healthcare. “We You’ll need ongoing training for your staff to improve your clinical documentation and avoid the following coding disasters. After time-consuming phone calls, staff found out why: The health plans were downcoding the diagnosis-related group (DRG).
Coding and clinical documentation have never been more important in healthcare. “We You’ll need ongoing training for your staff to improve your clinical documentation and avoid the following coding disasters. After time-consuming phone calls, staff found out why: The health plans were downcoding the diagnosis-related group (DRG).
In a hospital setting, nurses must be prepared for emergencies that can disrupt their carefully planned schedules. Nurses often have to care for multiple patients simultaneously, each with their unique needs and treatments. This can make it difficult to allocate time effectively and ensure that each patient receives the care they need.
Note: CMS documents how each ICD-10 code can be either a CC or MCC here. While many doctors naturally believe their patients require the highest level of care, DRGs provide an objective assessment. Documentation is crucial for assigning the correct DRG and, consequently, a realistic SOI score.
These include increased productivity, reduced paperwork, accurate documentation , and enhanced data security. By leveraging technology, clinicians can deliver better patient care and optimize their financial performance. The key is to understand the benefits it offers to the practice.
Key Improvements Implemented in 2024: Custom form builder allowing you to create and customize consent forms and documents tailored to your practices needs New, tailored treatment plan templates for specific payer requirements and modalities and improved treatment plan workflows to streamline your documentation and track patient progress in real time (..)
The potential overall cost savings and improvement in post-natal outcomes associated with such a reduction are well-documented and would be staggering. This is not a picayune academic point.
In nursing school, you studied and read like a madperson, wrote careplans (sorry to bring that up), learned to apply the nursing process (you may be sorry I brought that up), and turned your non-nurses mind into a nurse’s mind.
This case caught our attention because of its potential impact on plan design and plan administration of its mental health and substance use disorder (collectively “behavioral health”) benefits. Judge Block’s statement is particularly significant in light of health plans’ use of internally developed medical necessity criteria.
By providing practitioners with pre-written, customizable content, the planners make it possible to reduce time spent on documentation , allowing for more focus on direct patient care. The standardized approach promotes continuity of care even when multiple providers are involved.
Strategies to improve wound care and reduce readmissions To better align wound care practices with TEAM expectations, hospitals should consider the following targeted strategies: Integrate wound care tracking into EHRs Use validated tools like the Pressure Ulcer Scale for Healing (PUSH Tool) to assess wound healing progress.
Hospices should also be concerned about care coordination. The Centers for Medicare and Medicaid Services (CMS) is ramping up survey scrutiny for hospice this year, training surveyors to focus on interdisciplinary group careplanning and coordination of care as part of an emphasis on meeting four core Conditions of Participation.
An EHR migration can sometimes turn into a nightmare despite carefulplanning. The transition from one electronic health record (EHR) system to another can be fraught with challenges, leading to disruptions in workflow, productivity, and patient care.
Promoting a culture of knowledge and awareness of current standards of wound care. Providing consistent, evidence-based care and thorough documentation. Avoiding penalties and legal risks that go along with inaccurate assessments, incomplete documentation, and preventable pressure injuries. Minimize Risk and Liability.
Enhanced Patient Outcomes With access to a better organized and up-to-date health history, clinicians can tailor careplans to each patient’s unique needs, leading to better health outcomes. Continuous monitoring and updating of treatment plans ensure that patients receive the most appropriate and effective care.
Healthcare providers can help by educating patients on how to interpret these documents so that patients are fully aware of their financial responsibilities and can make better informed healthcare planning decisions. Explanation of Benefits (EOB): Understanding an EOB can be complex due to medical codes and insurance jargon.
Because your organization’s hiring practices are the first step toward improving your organization’s diversity, make sure to to carefully plan out and document these processes for fairness and inclusion. One policy to make explicit is prohibiting nepotism or favoritism in hiring. Watch for Unconscious Bias and Tokenism.
Unfortunately, many primary care professionals don’t anticipate that dementia will become a terminal condition and don’t start the process of advance careplanning early in the disease trajectory. For instance, what are the plans for nutrition when the person with dementia has difficulties eating or drinking?
By incorporating care coordination practices such as risk assessment, careplanning, care transitions, patient education, patient navigation, telehealth, and home visits, care coordination teams can bring in resources to help patients navigate health concerns that span physical, behavioral, and social risk factors and needs.
We will delve in to the complex and sensitive decisions faced by healthcare professionals as they strive to provide compassionate and dignified care to their residents. Preserving Dignity: Offering residents options for personalized careplans, respecting their wishes for pain management, comfort measures, and spiritual support.
You can provide consistent care if you have accurate documentation of your patient’s care at the hospital. Careplanning starts with an assessment and documentation of the wound. Diagnosing wounds correctly is critical for the best patient outcomes and accurate documentation for reimbursement purposes.
Why It Matters Enhanced Patient Care: Continuous, accurate data from integrated devices empowers clinicians to detect early warning signs, adjust treatments on the fly, and deliver personalized careplans. Enhanced Workflow Efficiency Manual data entry is labor-intensive and prone to errors.
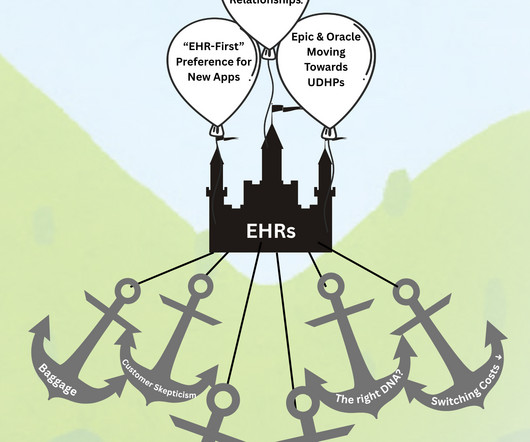
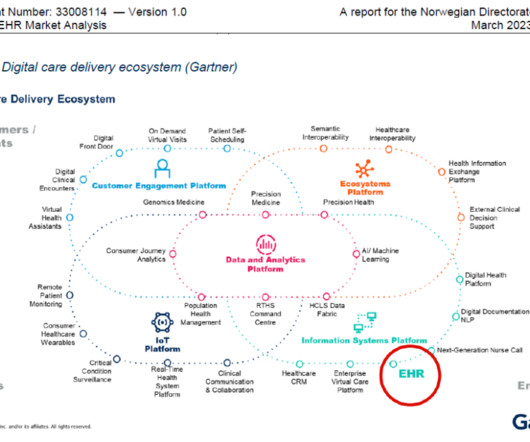
But as noted earlier, the roots of todays EHRs are as systems of record to document claims submissions. Betters UDHP is the underlying technology supporting the OneLondon shared careplanning solution across the city of London. In the short- to medium-term, UDHPs will be complementary to EHRs.
Having concluded that the closed panel, capitated integrated care system model could not be reached in a single impossible transformation, as the Clintons attempted and failed to do, it would sow the seeds of capitation through a managed care lite model called Accountable Care Organizations.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content